
Sunday, 15 July 2012
Guttate psoriasis

- distinctive acute eruption of small, drop-like, 1-10mm in diameter, salmon-pink papules, usually with a fine scale
- URTI from group A beta-hemolytic streptococci often precedes the eruption by 2-3 weeks
- primarily occurs on trunk and proximal extremities
Tuesday, 10 July 2012
Neuralgic amyotrophy
- a.k.a brachial neuritis, Parsonage-Turner syndrome, immune-mediated brachial plexus neuropathy (IBPN)
- occurs in response to bodily stress (surgery, flu, post vaccination)
- usually presents with an acute onset of severe pain in shoulder region
- intense pain usually last several days to weeks, but dull ache can persist
- as the pain dissipates, weakness and often sensory loss are appreciated
- scapular winging in common
- empirical treatment of severe pain with glucocorticoids is often used in the acute period
- this condition is usually self limiting (improve over weeks to months)

- occurs in response to bodily stress (surgery, flu, post vaccination)
- usually presents with an acute onset of severe pain in shoulder region
- intense pain usually last several days to weeks, but dull ache can persist
- as the pain dissipates, weakness and often sensory loss are appreciated
- scapular winging in common
- empirical treatment of severe pain with glucocorticoids is often used in the acute period
- this condition is usually self limiting (improve over weeks to months)
Monday, 9 July 2012
Orbital apex syndrome
- a.k.a Jacod syndrome
- collection of cranial nerve deficits associated with a mass lesion near the orbital apex region
- presents with proptosis, chemosis, optic neuropathy, Horner's syndrome, ophthalmoplegia, involvement of ophthalmic nerve (first branch of trigeminal nerve)

- collection of cranial nerve deficits associated with a mass lesion near the orbital apex region
- presents with proptosis, chemosis, optic neuropathy, Horner's syndrome, ophthalmoplegia, involvement of ophthalmic nerve (first branch of trigeminal nerve)


Friedreich ataxia
- autosomal recessive trinucleotide repeat disorder (GAA repeat)
- most common form of hereditary ataxia
- mutation in gene encoding protein frataxin on chromosome 9
- presents with progressive ataxia, cerebellar dysfunction, pyramidal weakness and sensory motor neuropathy
- other features: pes cavus, optic atrophy, hypertrophic cardiomyopathy (50-70% patients)
- most common form of hereditary ataxia
- mutation in gene encoding protein frataxin on chromosome 9
- presents with progressive ataxia, cerebellar dysfunction, pyramidal weakness and sensory motor neuropathy
- other features: pes cavus, optic atrophy, hypertrophic cardiomyopathy (50-70% patients)
Saturday, 7 July 2012
Alveolar-arterial gradient (A-a gradient)




Calculated A-a gradient = 150mmHg - PaCO2/0.8 - PaO2
Expected A-a gradient = Age/4 + 4
Normal A-a gradient suggest hypoventilation (hypoxia proportional to low ventilatory effort)
Increased A-a gradient suggest defect in diffusion, V/Q mismatch or right-left shunt
Friday, 6 July 2012
Monod's sign

Monod's sign: opacity surrounded by a crescent of air
- typical of aspergilloma (mycetoma) in a pre-existing air cavity (old tuberculosis, histoplasmosis, sarcoidosis, neoplasm)
Thursday, 5 July 2012
Hereditary neuropathy
- Charcot Marie Tooth (CMT) disease is the most common type of hereditary neuropathy
CMT type 1 (AD)
- usually presents in the first to third decade of life with distal leg weakness (eg: footdrop)
- muscle stretch reflexes are unobtainable or reduced throughout
- pes cavus
- often atrophy of muscles below knee (inverted champagne bottle leg)
- nerve conduction is very reduced
CMT type 2 (AD)
- tends to present later in life compared to type 1 and much milder
- nerve conduction is only very slightly reduced or normal
CMT type 3 / Dejerine Sottas (AR)
- presenting in infancy or early childhood
- affected children are severely weak
- typically associated with enlargement of peripheral nerves

CMT type 1 (AD)
- usually presents in the first to third decade of life with distal leg weakness (eg: footdrop)
- muscle stretch reflexes are unobtainable or reduced throughout
- pes cavus
- often atrophy of muscles below knee (inverted champagne bottle leg)
- nerve conduction is very reduced
CMT type 2 (AD)
- tends to present later in life compared to type 1 and much milder
- nerve conduction is only very slightly reduced or normal
CMT type 3 / Dejerine Sottas (AR)
- presenting in infancy or early childhood
- affected children are severely weak
- typically associated with enlargement of peripheral nerves
Wednesday, 4 July 2012
Actinomycosis
- indolent, slowly progressive infection caused by anaerobic or microaerophilic bacteria
- most commonly caused by A.israelii
- in vivo growth of actinomycetes usually results in the formation of characteristic clumps called grains or sulfur granules
- occurs most frequently at an oral, cervical or facial site as soft tissue swelling, abscess or mass lesion that is often mistaken for a neoplasm
- abdominal and pelvic actinomycosis usually follows introduction of organism through surgery or IUCD
- thoracic actinomycosis usually follows an indolent progressive course with involvement of pulmonary parenchyma and/or pleural space
- treatment: high dose IV benzylpenicillin and surgical resection/drainage

- most commonly caused by A.israelii
- in vivo growth of actinomycetes usually results in the formation of characteristic clumps called grains or sulfur granules
- occurs most frequently at an oral, cervical or facial site as soft tissue swelling, abscess or mass lesion that is often mistaken for a neoplasm
- abdominal and pelvic actinomycosis usually follows introduction of organism through surgery or IUCD
- thoracic actinomycosis usually follows an indolent progressive course with involvement of pulmonary parenchyma and/or pleural space
- treatment: high dose IV benzylpenicillin and surgical resection/drainage
Cheiroarthropathy
- condition of limited joint mobility that occur in diabetics
- characterised by thickening of skin resulting in contracture of fingers
- unable to extend the fingers to fully flatten the hand
- treatment: pain relieve, phystiotherapy, tight glycemic control
familial hypercholesterolemia
- type IIA hyperlipidemia
- autosomal codominant disorder characterised by elevated plasma levels of LDL-C with normal triglyceride, tendon xanthomas and premature coronary atherosclerosis
- homozygous FH occurs in approximately 1 in 1 million persons worldwide, whereas heterozygous FH occurs in 1 in 500 persons
- most homozygous FH present in childhood with cutaneous xanthomas on hand, wrist, elbows, knees, heels, or buttocks. Total cholesterol levels are usually >500mg/dL and devastating complication of homozygous FH is accelerated atherosclerosis
- treatment for FH is LDL apheresis (homozygous) and statin in combination with cholesterol absorption inhibitor
- family history is usually positive for premature atherosclerotic cardiovascular disease

- autosomal codominant disorder characterised by elevated plasma levels of LDL-C with normal triglyceride, tendon xanthomas and premature coronary atherosclerosis
- homozygous FH occurs in approximately 1 in 1 million persons worldwide, whereas heterozygous FH occurs in 1 in 500 persons
- most homozygous FH present in childhood with cutaneous xanthomas on hand, wrist, elbows, knees, heels, or buttocks. Total cholesterol levels are usually >500mg/dL and devastating complication of homozygous FH is accelerated atherosclerosis
- treatment for FH is LDL apheresis (homozygous) and statin in combination with cholesterol absorption inhibitor
- family history is usually positive for premature atherosclerotic cardiovascular disease
Saturday, 30 June 2012
Erythema gyratum repens

- characteristic concentric erythematous bands forming a wood-grain appearance
- associated with malignancy in up to 80% of patients
- most develop the eruption before the symptoms of malignancy
POEMS syndrome
- rare multisystem disease that occurs in the setting of plasma cell dyscrasia
- P - polyneuropathy (symmetrical and distal)
O - organomegaly (liver, spleen and lymph nodes)
E - endocrinopathy
M - monoclonal gammopathy
S - skin abnormalities (hyperpigmentation and hypertrichosis)
Sunday, 24 June 2012

Saturday, 23 June 2012
Warfarin reversal guideline

Warfarin reversal: consensus guidelines, on behalf of the Australasian Society of Thrombosis and Haemostasis. MJA 2004
Thursday, 21 June 2012

Tuesday, 19 June 2012
Ethylene glycol poisoning
- commonly used as a coolant and preservative and is found in polishes and detergents

- ethylene glycol poisoning often exhibits three distinct clinical phases after ingestion due to toxic metabolites glycolate, glyoxalate and oxalate
- first 12 hours - CNS effect predominate, patient appears intoxicated
- 12-24 hours - cardiopulmonary effect predominate, tachycardia, tachypnea and raised BP are common
- 24-72 hours - renal effects predominate
- hypocalcemia may result from precipitation of calcium oxalate in tissues and may be severe enough to cause tetany and typical ECG changes
- high anion gap metabolic acidosis
- treatment: gastric lavage within 1 hour of ingestion
- inhibit metabolism with intravenous ethanol (competitive inhibitor of alcohol dehydrogenase). Ethanol requires treatment on the ITU because of risk of respiratory depression
- fomepizole is an alternative treatment, being more potent than ethanol but generally more expensive
Sunday, 10 June 2012
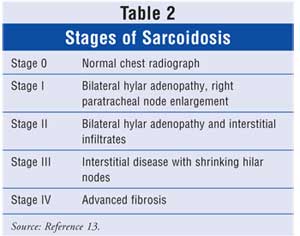
Sarcoidosis
- multisystem granulomatous disorder of unknown cause
- prevalence highest in Northern Europe
- 20-40% asymptomatic, discovered incidentally after routine CXR
- acute sarcoidosis presents with erythema nodosum and polyarthralgia which resolves spontaneously
- serum ACE elevated in 60% of patients, presumably reflecting macrophage activity
- transbronchial biopsy provide positive histology in 80% of patients
- Kveim reaction, a granulomatous reaction appearing 4 weeks after intradermal injection of sarcoid spleen or lymph node extract is positive in 50-60% of patients
- Mikulicz syndrome : sarcoidosis with parotid gland enlargement
- Heerfordt's syndrome (uveoparotid fever) : Mikulicz syndrome with acute uveitis and facial nerve palsy



Saturday, 9 June 2012
Refsum's disease
- autosomal recessive disorder
- caused by defective alpha oxidation of phytanic acid leading to its accumulation in tissues
- onset normally in late teens or 20s
- characterised by sensorimotor peripheral neuropathy, sensorineural deafness, anosmia, cerebellar ataxia, pes cavus, night blindness (retinitis pigmentosa), cardiac conduction abnormalities, epiphyseal dysplasia (shortening of 4th toe)
- elevated serum phytanic acid level
- treatment: dietary restriction of foods containing phytanic acid (chlorophyll)

- caused by defective alpha oxidation of phytanic acid leading to its accumulation in tissues
- onset normally in late teens or 20s
- characterised by sensorimotor peripheral neuropathy, sensorineural deafness, anosmia, cerebellar ataxia, pes cavus, night blindness (retinitis pigmentosa), cardiac conduction abnormalities, epiphyseal dysplasia (shortening of 4th toe)
- elevated serum phytanic acid level
- treatment: dietary restriction of foods containing phytanic acid (chlorophyll)
Thursday, 7 June 2012
Dextrocardia

ECG findings of dextrocardia
- right axis deviation
- positive QRS complex in aVR
- lead I : global negativity (inversion of all complexes)
- absent R wave progression in chest leads (dominant S wave throughout)

von Willebrand disease
- most common inherited bleeding disorder
- VWF serves two roles
i) major adhesion molecule that tethers the platelet to exposed subendothelium
ii) binding protein for FVIII
- males and females are equally affected but disease manifestation is more obvious in female due to menstruation and associated menorrhagia
- screening test are PT, APTT, factor VIII activity, vWF activity and vWF antigen level determination
- ristocetin is an antibiotic that causes vWF to bind to and activate platelet causing platelet agglutination. Degree of platelet agglutination is proportional to concentration of plasma vWF

- VWF serves two roles
i) major adhesion molecule that tethers the platelet to exposed subendothelium
ii) binding protein for FVIII
- males and females are equally affected but disease manifestation is more obvious in female due to menstruation and associated menorrhagia
- screening test are PT, APTT, factor VIII activity, vWF activity and vWF antigen level determination
- ristocetin is an antibiotic that causes vWF to bind to and activate platelet causing platelet agglutination. Degree of platelet agglutination is proportional to concentration of plasma vWF
Trigeminal neuralgia
- a.k.a tic douloureux
- incidence: 4.5 per 100,000 individuals
- characterised by excruciating paroxysms of pain in the lips, gums, cheek or chin (maxillary and mandibular branches, rarely ophthalmic branch)
- pain seldom last more than a few seconds or a minute or two
- may occur spontaneously or with speaking, chewing or smiling
- essential feature: objective signs of sensory loss cannot be demonstrated on examination
- symptoms result from ectopic generation of action potentials in pain sensitive afferent fibres of 5th cranial nerve roots just before it enters the lateral surface of the pons
- treatment: carbamazepine 100mg od increased gradually to maintenance dose of 200mg qid, alternative is oxcarbazepine 300-1200mg bd
- if medical treatment fails, consider microvascular decompression
- incidence: 4.5 per 100,000 individuals
- characterised by excruciating paroxysms of pain in the lips, gums, cheek or chin (maxillary and mandibular branches, rarely ophthalmic branch)
- pain seldom last more than a few seconds or a minute or two
- may occur spontaneously or with speaking, chewing or smiling
- essential feature: objective signs of sensory loss cannot be demonstrated on examination
- symptoms result from ectopic generation of action potentials in pain sensitive afferent fibres of 5th cranial nerve roots just before it enters the lateral surface of the pons
- treatment: carbamazepine 100mg od increased gradually to maintenance dose of 200mg qid, alternative is oxcarbazepine 300-1200mg bd
- if medical treatment fails, consider microvascular decompression
Monday, 28 May 2012
Babesiosis
- tick-borne malaria-like illness caused by parasite of genus Babesia
- Babesia microti is the cause of babesiosis in northeastern United States
- intraerythrocytic Babesia destroy the red blood cells causing hemolytic anemia and hemoglobinuria
- mild illness presents with malaise, fatigue, weakness, fever, chills, sweat, headache, myalgia, anorexia, dry cough, arthralgia and nausea
- post-splenectomy, HIV, malignancy and immunosuppression are at risk of severe illness
- symptoms are greater with higher percentage of parasitism
- diagnosed by microscopic examination of Giemsa-stained thin blood smears - round or pear-shaped organism
- asymptomatic need not be treated
- mild illness: oral atovaquone + azithromycin for 7 - 10 days
- severe illness: IV clindamycin + oral quinine for 7 - 10 days

- Babesia microti is the cause of babesiosis in northeastern United States
- intraerythrocytic Babesia destroy the red blood cells causing hemolytic anemia and hemoglobinuria
- mild illness presents with malaise, fatigue, weakness, fever, chills, sweat, headache, myalgia, anorexia, dry cough, arthralgia and nausea
- post-splenectomy, HIV, malignancy and immunosuppression are at risk of severe illness
- symptoms are greater with higher percentage of parasitism
- diagnosed by microscopic examination of Giemsa-stained thin blood smears - round or pear-shaped organism
- asymptomatic need not be treated
- mild illness: oral atovaquone + azithromycin for 7 - 10 days
- severe illness: IV clindamycin + oral quinine for 7 - 10 days
Stiff person syndrome
- spontaneous discharge of the motor neurons of the spinal cord cause involuntary muscle contractions mainly involving the axial (trunk) and proximal lower extremity muscles
- gait becomes more stiff and labored, with hyperlordosis of lumbar spine
- superimposed episodic muscle spasms are precipitated by sudden movements, unexpected noises and emotional upset
- serum antibodies against glutamic acid decarboxylase are present in approximately 2/3 of cases
- treatment is mostly palliative with muscle relaxant with potentiate GABA actions (such as benzodiazepines)

- gait becomes more stiff and labored, with hyperlordosis of lumbar spine
- superimposed episodic muscle spasms are precipitated by sudden movements, unexpected noises and emotional upset
- serum antibodies against glutamic acid decarboxylase are present in approximately 2/3 of cases
- treatment is mostly palliative with muscle relaxant with potentiate GABA actions (such as benzodiazepines)
Saturday, 26 May 2012
Calciphylaxis
- calcific uremic arteriolopathy seen almost exclusively in patients with advanced CKD
- heralded by livedo reticularis and advances to patches of ischemic necrosis especially on the legs, thighs, abdomen and breasts
- pathologically, there is vascular occlusion associated with extensive vascular (calcification of tunica media) and soft tissue calcification
- warfarin is a risk factor of calciphylaxis ( because warfarin decrease vitamin K dependent regeneration of matrix GLA protein which is important in preventing vascular calcification)
- optimal treatment is prevention, with rigorous and continuous control of phosphate and calcium balance
- no specific treatment

- heralded by livedo reticularis and advances to patches of ischemic necrosis especially on the legs, thighs, abdomen and breasts
- pathologically, there is vascular occlusion associated with extensive vascular (calcification of tunica media) and soft tissue calcification
- warfarin is a risk factor of calciphylaxis ( because warfarin decrease vitamin K dependent regeneration of matrix GLA protein which is important in preventing vascular calcification)
- optimal treatment is prevention, with rigorous and continuous control of phosphate and calcium balance
- no specific treatment
Allergic interstitial nephritis (AIN)
- classically presents with fever, rash, peripheral eosinophilia and oliguric renal failure after 7 - 10 days treatment with methicillin or another B-lactam antibiotics
- atypical reactions can occur with NSAIDs in which fever, rash and eosinophilia are rare but acute renal failure with heavy proteinuria is common
- urinalysis reveal pyuria with white blood cell casts and hematuria
- renal biopsy usually not required for diagnosis but reveals extensive interstitial and tubular infiltration of leukocytes, including eosinophils
- discontinuation of offending agent often leads to reversal of renal injury
- atypical reactions can occur with NSAIDs in which fever, rash and eosinophilia are rare but acute renal failure with heavy proteinuria is common
- urinalysis reveal pyuria with white blood cell casts and hematuria
- renal biopsy usually not required for diagnosis but reveals extensive interstitial and tubular infiltration of leukocytes, including eosinophils
- discontinuation of offending agent often leads to reversal of renal injury
Atrial fibrillation

- Should look for AF in patient who presents with dyspnea, palpitation, syncope/dizziness, chest discomfort, stroke/TIA
- In patient with permanent AF who need treatment for rate control, beta blocker or rate-limiting CCB should be preffer initial monotherapy, digoxin is considered in predominantly sedentary patient
- In patient with persistent AF considered for pharmacological cardioversion, Class Ic drug (flecainide or propafenone) should be drug of choice in the absence of structural heart disease and amiodarone in the presence of structural heart disease
- rate control strategy should be the preferred initial option in persistent AF patient with
~ age over 65
~ coronary heart disease
~ with contraindication to antiarrhythmic drug
~ unsuitable for cardioversion
~ without congestive heart failure
- rhythm control strategy should be the preferred initial option in persistent AF patient with
~ younger patient
~ symptomatic
~ presenting for first time with lone AF
~ those with AF secondary to a treated/corrected precipitant
~ with congestive heart failure
- patient should be maintained on therapeutic anticoagulation with warfarin to keep INR between 2.0-3.0 for minimum of 3 weeks before cardioversion and 4 weeks after cardioversion


Reference: NICE clinical guideline 36 Atrial fibrillation
Carotid sinus hypersensitivity (CSH)
- exaggerated response to carotid sinus stimulation
- diagnosis is made after ischemic heart disease and rhythm disturbance is excluded
- CSH may be predominantly cardioinhibitory (resulting in bradycardia), vasodepressor (resulting in hypotension) or mixture of both
- presents with recurrent dizziness, near syncope, syncope, unexplained falls (drop attacks), symptoms produced when wearing tight-fitting collar clothes or when taking carotid pulse
- cardioinhibitory CSH is managed with insertion of dual-chamber pacemaker and vasodilatory CSH is managed with support stocking, fludrocortisone and midodrine (alpha-1 agonist)
- diagnosis is made after ischemic heart disease and rhythm disturbance is excluded
- CSH may be predominantly cardioinhibitory (resulting in bradycardia), vasodepressor (resulting in hypotension) or mixture of both
- presents with recurrent dizziness, near syncope, syncope, unexplained falls (drop attacks), symptoms produced when wearing tight-fitting collar clothes or when taking carotid pulse
- cardioinhibitory CSH is managed with insertion of dual-chamber pacemaker and vasodilatory CSH is managed with support stocking, fludrocortisone and midodrine (alpha-1 agonist)
Friday, 25 May 2012
Adult onset Still disease
- rare form of inflammatory arthritis
- begins after the age of 16 years
- diagnosis of exclusion
- serum ferritin is usually elevated
- RF and ANA are classically negative
- treatment: NSAIDs
- Yamaguchi's criteria

- begins after the age of 16 years
- diagnosis of exclusion
- serum ferritin is usually elevated
- RF and ANA are classically negative
- treatment: NSAIDs
- Yamaguchi's criteria
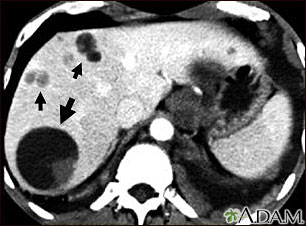
Echinococcosis
- infection caused by larval stage of Echinococcus granulosus complex (dog tapeworm), which produce unilocular cystic lesion
- slowly enlarging echinococcal cyst generally remain asymptomatic until their expanding size or their space occupying effect in an involved organ (commonly liver and lungs) elicits symptomss
- hydatid liver disease presents with right upper quadrant pain, palpable mass in right upper quadrant or bile duct compression resulting in jaundice
- calcification is often seen on abdominal X ray and ultrasound is excellent means of demonstrating the cyst
- the most pathognomonic finding if demonstrable is that of daughter cysts within the larger cyst
- diagnostic aspiration is not usually recommended because of risk of fluid leakage resulting in either dissemination or infection or anaphylactic reaction
- treatment: Albendazole or PAIR (percutaneous aspiration, infusion of scolicidal agent and reaspiration), or pericystectomy for complicated cyst
- slowly enlarging echinococcal cyst generally remain asymptomatic until their expanding size or their space occupying effect in an involved organ (commonly liver and lungs) elicits symptomss
- hydatid liver disease presents with right upper quadrant pain, palpable mass in right upper quadrant or bile duct compression resulting in jaundice
- calcification is often seen on abdominal X ray and ultrasound is excellent means of demonstrating the cyst
- the most pathognomonic finding if demonstrable is that of daughter cysts within the larger cyst
- diagnostic aspiration is not usually recommended because of risk of fluid leakage resulting in either dissemination or infection or anaphylactic reaction
- treatment: Albendazole or PAIR (percutaneous aspiration, infusion of scolicidal agent and reaspiration), or pericystectomy for complicated cyst
Thursday, 24 May 2012
Yersiniosis
- zoonotic infection with an enteropathogenic Yersinia species (Yersinia enterocolitica or Yersinia pseudotuberculosis)
- presents with abdominal pain and diarrhea
- can present with pseudoappendicitis (mesenteric adenitis)
- initial replication in small intestine is followed by invasion of Peyer's patches of distal ileum via M cells with onward spread to mesenteric lymph nodes
- gold standard for diagnosis is serology
- most cases of diarrhea are self limiting
- fluoroquinolone therapy is effective for bacteremia in adults

- presents with abdominal pain and diarrhea
- can present with pseudoappendicitis (mesenteric adenitis)
- initial replication in small intestine is followed by invasion of Peyer's patches of distal ileum via M cells with onward spread to mesenteric lymph nodes
- gold standard for diagnosis is serology
- most cases of diarrhea are self limiting
- fluoroquinolone therapy is effective for bacteremia in adults
Wednesday, 23 May 2012
Relapsing polychondritis
- characterised by inflammation of cartilage (ear, nose and laryngotracheobronchial tree)
- also manifested with scleritis, neurosensory hearing loss, polyarthritis, cardiac abnormalitis, skin lesion and glomerulonephritis
- most common in 5th decade
- systemic features such as fever, fatigue and weight loss precede the clinical signs by several weeks
- auricular chondritis is the most frequent presenting manifestation (40%), and eventually affecting 85% of patients
- typically involving pinna of ears and sparing earlobe because they do not contain cartilage
- treatment: prednisolone 40-60mg/day

- also manifested with scleritis, neurosensory hearing loss, polyarthritis, cardiac abnormalitis, skin lesion and glomerulonephritis
- most common in 5th decade
- systemic features such as fever, fatigue and weight loss precede the clinical signs by several weeks
- auricular chondritis is the most frequent presenting manifestation (40%), and eventually affecting 85% of patients
- typically involving pinna of ears and sparing earlobe because they do not contain cartilage
- treatment: prednisolone 40-60mg/day
Achalasia
- caused by loss of ganglion cells within the esophageal myenteric plexus
- incidence 1:100,000
- presents at age between 25 and 60 years
- defined as reduced or absence of peristalsis and failure of lower esophageal sphincter to relax when swallowing
- presents with dysphagia, regurgitation, chest pain (esophageal spasm) and weight loss
- patient with advanced achalasia are at risk for bronchitis, pneumonia or lung abscess from chronic regurgitation and aspiration
- differential diagnoses are diffuse esophageal spasm (DES), Chagas' disease and pseudoachalasia (tumor infiltration)
- diagnosed by barium swallow X ray (dilated esophagus with poor emptying and air fluid level, tapering at the LES giving a beak-like appearance) and esophageal manometry (impaired LES relaxation and absent peristalsis)
- treatment: endoscopic pneumatic dilatation of LES (efficacy 32-98%), intra-sphincteric injection of botulinum toxin or Heller's cardiomyotomy
- increased risk of esophageal squamous cell cancer secondary to prolonged stasis esophagitis

- incidence 1:100,000
- presents at age between 25 and 60 years
- defined as reduced or absence of peristalsis and failure of lower esophageal sphincter to relax when swallowing
- presents with dysphagia, regurgitation, chest pain (esophageal spasm) and weight loss
- patient with advanced achalasia are at risk for bronchitis, pneumonia or lung abscess from chronic regurgitation and aspiration
- differential diagnoses are diffuse esophageal spasm (DES), Chagas' disease and pseudoachalasia (tumor infiltration)
- diagnosed by barium swallow X ray (dilated esophagus with poor emptying and air fluid level, tapering at the LES giving a beak-like appearance) and esophageal manometry (impaired LES relaxation and absent peristalsis)
- treatment: endoscopic pneumatic dilatation of LES (efficacy 32-98%), intra-sphincteric injection of botulinum toxin or Heller's cardiomyotomy
- increased risk of esophageal squamous cell cancer secondary to prolonged stasis esophagitis
Tuesday, 22 May 2012
Antidotes
| Agent | Indication |
|---|---|
| Activated charcoal with sorbital | used for many oral toxins |
| Adenosine | Theophylline antidote for adenosine poisoning |
| Atropine | organophosphate and carbamate insecticides,nerve agents, some mushrooms |
| Beta blocker | theophylline |
| Calcium chloride | calcium channel blockers, black widow spider bites |
| Calcium gluconate | hydrofluoric acid |
| Chelators such as EDTA, dimercaprol (BAL), penicillamine, and 2,3-dimercaptosuccinic acid (DMSA, succimer) | heavy metal poisoning |
| Cyanide antidote (amyl nitrite, sodium nitrite, or thiosulfate) | cyanide poisoning |
| Cyproheptadine | serotonin syndrome |
| Deferoxamine mesylate | Iron poisoning |
| Digoxin Immune Fab antibody (Digibind and Digifab) | digoxin poisoning |
| Diphenhydramine hydrochloride and benztropine mesylate | Extrapyramidal reactions associated withantipsychotic |
| Ethanol or fomepizole | ethylene glycol poisoning and methanol poisoning |
| Flumazenil | benzodiazepine poisoning |
| Glucagon | beta blocker poisoning and calcium channel blockerpoisoning |
| 100% oxygen or hyperbaric oxygen therapy (HBOT) | carbon monoxide poisoning and cyanide poisoning |
| Insulin | beta blocker poisoning and calcium channel blockerpoisoning |
| Leucovorin | methotrexate and trimethoprim |
| Methylene blue | treatment of conditions that cause methemoglobinemia |
| Naloxone hydrochloride | opioid poisoning |
| N-acetylcysteine | Paracetamol (acetaminophen) poisoning |
| Octreotide | oral hypoglycemic agents |
| Pralidoxime chloride (2-PAM) | organophosphate insecticides, followed after atropine |
| Protamine sulfate | Heparin poisoning |
| Prussian blue | Thallium poisoning |
| Physostigmine sulfate | anticholinergic poisoning |
| Pyridoxine | Isoniazid poisoning, ethylene glycol |
| Phytomenadione (vitamin K) and fresh frozen plasma | warfarin poisoning and indanedione |
| Sodium bicarbonate | ASA, TCAs with a wide QRS |
Monday, 21 May 2012
Water deprivation test
- Patients are deprived of fluid for 8 hours or until 5% of body weight is loss
- patient should be weighed hourly
- plasma osmolality is measured 4 hourly
- urine volume and osmolality 2 hourly
- then give 2microgram desmopressin IM and check urine volume & osmolality and plasma osmolality over next 4 hours
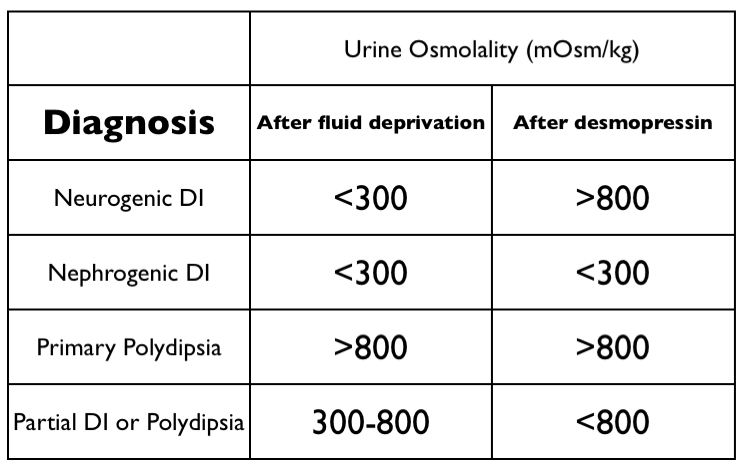
- Interpretation
~ if serum osmolality > 305 mOsmol/kg = diabetes insipidus
~ urine osmolality < 300 mOsmol/kg after fluid deprivation and rising to above 800mOsmol/kg after desmopressin = cranial diabetes insipidus
~ urine osmolality < 300 mOsmol/kg after fluid deprivation and remains < 300mOsmol/kg after desmopressin = nephrogenic diabetes insipidus
~ urine osmolality > 800 mOsmol/kg after fluid deprivation without desmopressin = primary polydipsia
~ urine osmolality between 300 and 800 mOsmol/kg = partial DI/polydipsia
- patient should be weighed hourly
- plasma osmolality is measured 4 hourly
- urine volume and osmolality 2 hourly
- then give 2microgram desmopressin IM and check urine volume & osmolality and plasma osmolality over next 4 hours
- Interpretation
~ if serum osmolality > 305 mOsmol/kg = diabetes insipidus
~ urine osmolality < 300 mOsmol/kg after fluid deprivation and rising to above 800mOsmol/kg after desmopressin = cranial diabetes insipidus
~ urine osmolality < 300 mOsmol/kg after fluid deprivation and remains < 300mOsmol/kg after desmopressin = nephrogenic diabetes insipidus
~ urine osmolality > 800 mOsmol/kg after fluid deprivation without desmopressin = primary polydipsia
~ urine osmolality between 300 and 800 mOsmol/kg = partial DI/polydipsia
Sunday, 20 May 2012
Takayasu's arteritis
- an inflammatory and stenotic disease of medium and large-sized arteries characterized by strong predilection for the aortic arch and its branches
- a.k.a aortic arch syndrome
- 2-3 per million
- 80% are women and mean age of onset is 30 years
- panarteritis with inflammatory mononuclear cell infiltrates and occasionally giant cells
- presents with fever, night sweats, arthralgia, anorexia and weight loss
- pulses are commonly absent in the involved vessels, particularly subclavian artery
- hypertension occurs in 32-93% of patients and contribute to renal, cardiac and cerebral injury
- diagnosis is confirmed by the characteristic pattern on arteriography which includes irregular vessel walls, stenosis, post stenotic dilatation, aneurysm formation, occlusion and evidence of increased collateral circulation
- corticosteroid with the addition of steroid sparing agents such as methotrexate or azathioprine are mainstay of treatment
- a.k.a aortic arch syndrome
- 2-3 per million
- 80% are women and mean age of onset is 30 years
- panarteritis with inflammatory mononuclear cell infiltrates and occasionally giant cells
- presents with fever, night sweats, arthralgia, anorexia and weight loss
- pulses are commonly absent in the involved vessels, particularly subclavian artery
- hypertension occurs in 32-93% of patients and contribute to renal, cardiac and cerebral injury
- diagnosis is confirmed by the characteristic pattern on arteriography which includes irregular vessel walls, stenosis, post stenotic dilatation, aneurysm formation, occlusion and evidence of increased collateral circulation
- corticosteroid with the addition of steroid sparing agents such as methotrexate or azathioprine are mainstay of treatment
Friday, 18 May 2012
Paroxysmal cold hemoglobinuria
- rare form of AIHA occuring mostly in children
- usually triggered by a viral infection, usually self limited
- characterised by the involvement of Donath-Landsteiner antibody
- in vitro, this antibody has unique serologic feature: it has anti-P specificity and it binds to red cells only at low temperature (optimally at 4°C). When temperature is shifted to 37°C, lysis of red cells take place in the presence of complement
- consequently, in vivo there is intravascular hemolysis resulting in hemoglobinuria
- also presents with rigor and bone pain
- supportive treatment inlcuding blood transfusion is needed to control the anemia

- usually triggered by a viral infection, usually self limited
- characterised by the involvement of Donath-Landsteiner antibody
- in vitro, this antibody has unique serologic feature: it has anti-P specificity and it binds to red cells only at low temperature (optimally at 4°C). When temperature is shifted to 37°C, lysis of red cells take place in the presence of complement
- consequently, in vivo there is intravascular hemolysis resulting in hemoglobinuria
- also presents with rigor and bone pain
- supportive treatment inlcuding blood transfusion is needed to control the anemia
Thursday, 17 May 2012
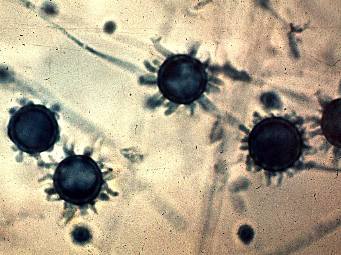
Histoplasmosis
- caused by Histoplasma capsulatum, a thermal dimorphic soil fungus
- a.k.a Darling's disease (Histoplasma discovered in 1905 by Darling)
- infection follows inhalation of microconidia. Once they reach the alveolar space, microconidia are rapidly recognised and engulfed by alveolar macrophages
- clinical spectrum of histoplasmosis ranges from asymptomatic infection (immunocompetent individuals with low level of exposure) to life threatening illness (immunocompromised - progressive disseminated histoplasmosis)
- it causes TB-like illness
- fungal culture remains the gold standard diagnostic test for histoplasmosis (Groccott stain)
- treatment is indicated for progressive disseminated histoplasmosis, chronic pulmonary histoplasmosis or symptomatic patients with acute pulmonary histoplasmosis
- drug: liposomal amphotericin B or itraconazole
- a.k.a Darling's disease (Histoplasma discovered in 1905 by Darling)
- infection follows inhalation of microconidia. Once they reach the alveolar space, microconidia are rapidly recognised and engulfed by alveolar macrophages
- clinical spectrum of histoplasmosis ranges from asymptomatic infection (immunocompetent individuals with low level of exposure) to life threatening illness (immunocompromised - progressive disseminated histoplasmosis)
- it causes TB-like illness
- fungal culture remains the gold standard diagnostic test for histoplasmosis (Groccott stain)
- treatment is indicated for progressive disseminated histoplasmosis, chronic pulmonary histoplasmosis or symptomatic patients with acute pulmonary histoplasmosis
- drug: liposomal amphotericin B or itraconazole
Subacute thyroiditis
- a.k.a De Quervain's /granulomatous / viral thyroiditis
- peak incidence 30-50 years, women affected 3 times more common than men
- during initial phase of follicular destrution, there is release of Tg and thyroid hormones, leading to increased circulating T4 and T3 and suppression of TSH (during this stage, radioactive iodine uptake is low or undetectable)
- after several weeks, the thyroid is depleted of stored thyroid hormone and a phase of hypothyroidism typically occurs
- finally thyroid hormone and TSH levels return to normal as disease subsides
- presents with painful and enlarged thyroid, sometimes fever
- malaise and URTI may precede the thyroid related features by several weeks
- patient typically complained of sore throat and pain is often radiated to jaw or ear
- ESR and CRP are markedly elevated
- treatment: NSAIDs (eg: aspirin 600mg QID), or prednisolone 40-60mg gradually tapered over 6-8 weeks
- thyroid function should be monitored every 2-4 weeks using TSH and unbound T4 levels

- peak incidence 30-50 years, women affected 3 times more common than men
- during initial phase of follicular destrution, there is release of Tg and thyroid hormones, leading to increased circulating T4 and T3 and suppression of TSH (during this stage, radioactive iodine uptake is low or undetectable)
- after several weeks, the thyroid is depleted of stored thyroid hormone and a phase of hypothyroidism typically occurs
- finally thyroid hormone and TSH levels return to normal as disease subsides
- presents with painful and enlarged thyroid, sometimes fever
- malaise and URTI may precede the thyroid related features by several weeks
- patient typically complained of sore throat and pain is often radiated to jaw or ear
- ESR and CRP are markedly elevated
- treatment: NSAIDs (eg: aspirin 600mg QID), or prednisolone 40-60mg gradually tapered over 6-8 weeks
- thyroid function should be monitored every 2-4 weeks using TSH and unbound T4 levels
Wednesday, 16 May 2012
Tardive dyskinesia
- developed months to years after initiation of neuroleptic medications
- choreiform movements involving mouth, lips and tongue
- abnormal movement may develop after stopping the offending agent
- atypical antipsychotics has lower risk of TD
- treatment consists of stopping the offending agent
- TD remits within 3 months of stopping the drug and most patients gradually improve over the course of several years
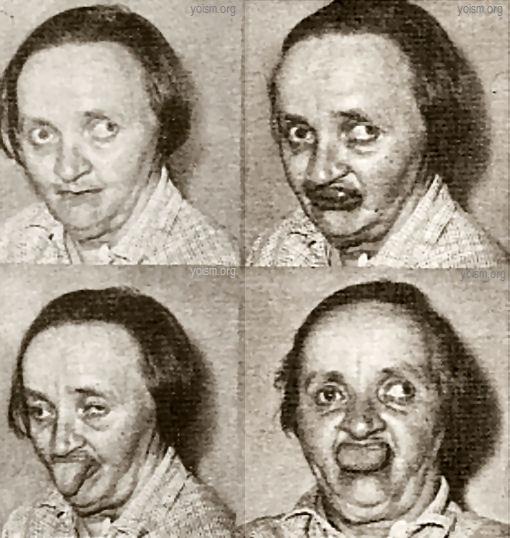
- choreiform movements involving mouth, lips and tongue
- abnormal movement may develop after stopping the offending agent
- atypical antipsychotics has lower risk of TD
- treatment consists of stopping the offending agent
- TD remits within 3 months of stopping the drug and most patients gradually improve over the course of several years
Sunday, 13 May 2012
Peripartum cardiomyopathy
- develops during the last trimester or within first 6 months after pregnancy
- between 1:3000 and 1:15,000 deliveries
- risk factors are increased maternal age, increased parity, twin pregnancy, malnutrition, tocolytics, and pre-eclampsia
- cause is unknown
- management is supportive with sodium restriction, digoxin, diuretics and vasodilators (eg:hydralazine)
- increased incidence of thrombosis and common to anticoagulate patient with heparin
- risk of recurrence in future pregnancy is 40%
- prognosis is reasonable with recovery of ventricular function in up to 50% patients

- between 1:3000 and 1:15,000 deliveries
- risk factors are increased maternal age, increased parity, twin pregnancy, malnutrition, tocolytics, and pre-eclampsia
- cause is unknown
- management is supportive with sodium restriction, digoxin, diuretics and vasodilators (eg:hydralazine)
- increased incidence of thrombosis and common to anticoagulate patient with heparin
- risk of recurrence in future pregnancy is 40%
- prognosis is reasonable with recovery of ventricular function in up to 50% patients
Loiasis
- filarial infection caused by Loa loa (African eye worm)
- transmitted by Chrysops fly
- adult parasites live in subcutaneous tissue
- microfilariae circulate in blood with a diurnal periodocity
- subconjunctival migration of an adult worm
- Calabar swelling (localised area of angioedema and erythema developing on extremities) is thought to result from a hypersensitivity reaction to adult worm antigens
- definitive diagnosis requires the detection of microfilariae in peripheral blood or isolation of adult worm from the eye or subcutaneous biopsy
- eosinophilia suggest the diagnosis
- diethylcarbamazine (DEC) for 3 weeks


- transmitted by Chrysops fly
- adult parasites live in subcutaneous tissue
- microfilariae circulate in blood with a diurnal periodocity
- subconjunctival migration of an adult worm
- Calabar swelling (localised area of angioedema and erythema developing on extremities) is thought to result from a hypersensitivity reaction to adult worm antigens
- definitive diagnosis requires the detection of microfilariae in peripheral blood or isolation of adult worm from the eye or subcutaneous biopsy
- eosinophilia suggest the diagnosis
- diethylcarbamazine (DEC) for 3 weeks
Subscribe to:
Posts (Atom)